Last week, the WHO’s governing body decided to put reform of the Member State Mechanism on Substandard and Falsified Medicines into the “too-hard-for-now” box. Reports on the decision inevitably spat out the “One in 10 medicines in low and middle income countries is substandard or falsified” trope. At the same time, politicians continued to fret about access to quality-assured medicines, urging measures to control costs.
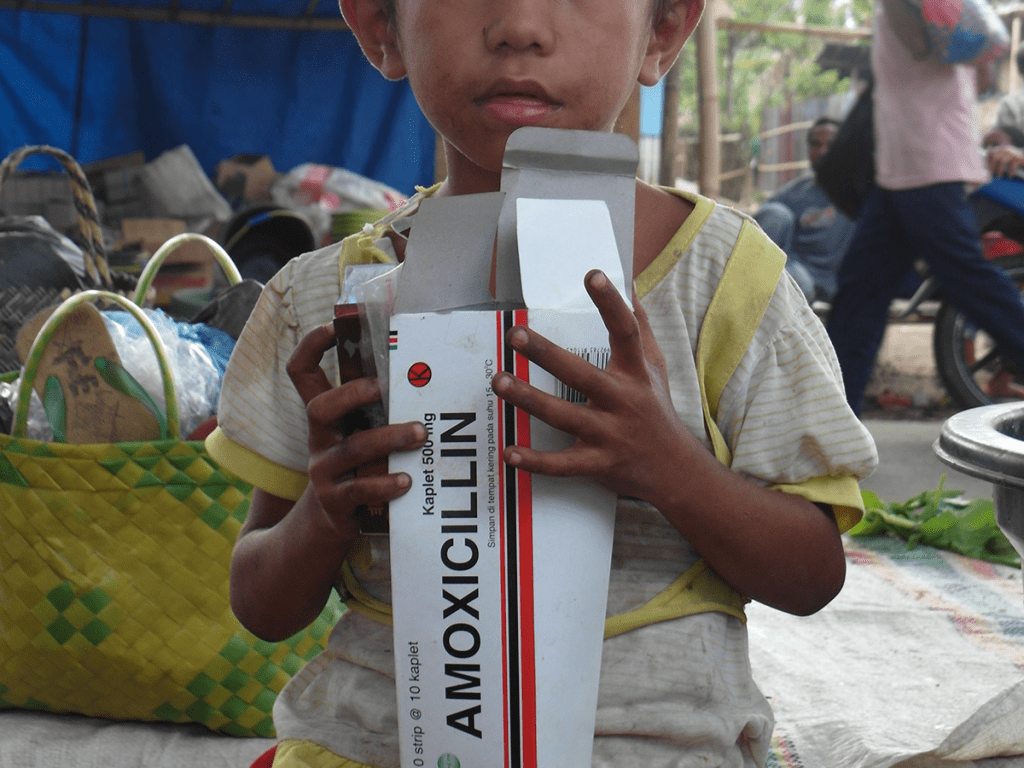
Also last week, the STARmeds group at Indonesia’s Universitas Pancasila published a large study looking at the affordability and quality of 5 essential medicines in Indonesia. It is a companion piece to a previously published study that measures the prevalence of substandard and falsified versions of these five medicines: two antibiotics (amoxicillin and cefixime), a hypertension drug (amlodipine), a steroid (dexamethasone) and a drug for gout (allopurinol). Importantly, the study adjusts the raw survey estimates using the market share of each individual brand of those medicines in the Indonesian market.
That small change, never before used in a survey of medicines collected from randomly-selected retail outlets and health-care settings, makes a huge difference. Headline prevalence came down by nearly half (47%). Why the big difference? Testing medicines is expensive, so researchers tend to avoid testing the same brand over and over. It’s more interesting to test lots of different brands. In the STARmeds study, we worked hard to get some pretty esoteric brands, especially on the internet.Most patients won’t work that hard; they’ll but the brand that is stocked in 9 out of 10 pharmacies. Just as well. It turns out those esoteric brands are more likely to fail testing. Apparently, good quality medicines sell better than poor quality medicines, at least in the world’s fourth most populous country. But here’s the thing: if you don’t adjust for this, then the esoteric but crappy brands used by a few thousand patients have the same weight in your study results as the common but just-fine brands (or unbranded generics) that are used by tens of millions. This means it is possible, even likely, that the unweighted studies that went into the WHO analysis leading to the famous “1 in 10” headline overestimated the true prevalence of poor quality medicines, at least in many of the large middle-income markets of Asia.
The newly-published pricing paper also confirms that in Indonesia, the cheapest medicines are just as likely to be good quality as the most expensive ones. This reaffirms findings of an earlier sister study of the quality and price of cardio-vascular and diabetes medicines in a single district of East Java carried out by colleagues at The George Institute and Universitas Brawijaya.
The variation in prices we found is eye-popping; Indonesian patients who can’t be bothered to queue at busy health facilities for free medicines can easily pay between 15 or 20 times as much for the most expensive brand as for the cheapest. The greediest sellers will often charge four or five times as much as their more modest colleagues even for the very same brand. And I guess that’s fine, as long as those who are paying the higher prices can afford to. One of the most important findings of the new STARmeds study was that in every region we visited, including some very remote rural areas across Indonesia’s 13,000 islands, we found that patients could easily find affordable versions of these frequently-prescribed medicines, costing less than a day’s earnings at the local minimum wage for a month’s supply, or a single therapeutic course.
Indonesia is a middle-income country with a solid health system, a lively pharmaceutical sector, and a strong medicine regulator. It certainly doesn’t represent all “LMICs”. But that’s partly my point. Of course it is important to draw attention to access challenges, and to the dangers posed by substandard and falsified medicines. But it is perhaps time to introduce some nuance, and some more robust methods, into our discussions, as well as in to long-lasting but inaccurate WHO press releases.
If you’re interested in this subject, you will find our entire dataset of 1,333 samples, with sample level pricing data and raw laboratory test results for the 1254 samples that were tested (identity, assay, dissolution, and where relevant uniformity of assay) as well as the analysis code used in the two papers mentioned, in the STARmeds study archive. Free to access, at https://dataverse.harvard.edu/dataverse/STARmeds. Please use responsibly!